The False Dichotomy of Drug Testing to Receive Welfare: Part 2
*Hay una versión español abajo
In the first part of this post, I discussed the seemingly nonsensical scheduling of certain drugs, primarily marijuana, LSD, psilocybin (magic mushrooms), and MDMA (ecstasy). All these drugs are Schedule I drugs, meaning that they are considered to have no medicinal value. However, organizations like the Multidisciplinary Association for Psychedelic Studies (MAPS) and John Hopkins have conducted and analyzed studies that claim otherwise.
This most evident miscatigorization of marijuana is the fact that medicinal marijuana is legalized in 33 states in the U.S. Additionally, John Hopkins School of Public Health also states that various studies have concluded that people with chronic pain who are treated with cannabinoid (the chemical found in marijuana) related products can experience significant pain reduction. This same pool of studies also indicated that short-term use of certain oral cannabinoid products helped improve symptoms of people with multiple sclerosis-related muscle spasms in addition to preventing chemotherapy-induced nausea and vomiting.
There is also much promise to psychedelics having medicinal properties. In 2014 MAPS published a study that showed evidence that LSD-assisted psychotherapy can possibly be used to treat anxiety in patients with life threatening diseases such as end-stage cancer. Later in 2016 John Hopkins and researchers from the New York University Langone Medical Center both published similar positive results of experiments using psilocybin to treat depression and anxiety in patients with life-threatening diseases. Two years previously John Hopkins had success using psilocybin to promote smoking cessation. Their study found that former smokers had an 80% abstinence rate after a 6 month period of monitored psilocybin use, compared to the 35% abstinence rate of varenicline, which is commonly viewed as the most effective drug for smoking cessation. Other treatments such as nicotine replacement and behavior therapies typically have a success rate of less than 30%. MAPS also completed another study in 2006 that showed psilocybin could be effective in helping patients with Obsessive-Compulsive Disorder (OCD) manage their symptoms. Last year MAPS also found promising results of using MDMA to treat PTSD, where 54% of the participants no longer fit the diagnostic criteria of PTSD after only 1-2 months sessions.
While the world is just now uncovering the “new” medicinal potential of psychedelics (well, new to westerners. Certain indigenous groups like Quechua and Mazatecs have already been using psychedelics like ayahuasca and psilocybin, respectively, for various healing purposes for quite some time now), there’s still the detrimental side of drugs, addiction, that most of the world is already familiar with. But what’s the best way to manage drug addiction? Portugal might have the answer.
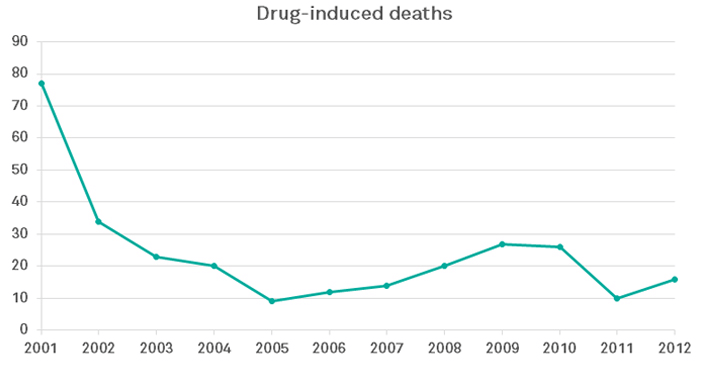
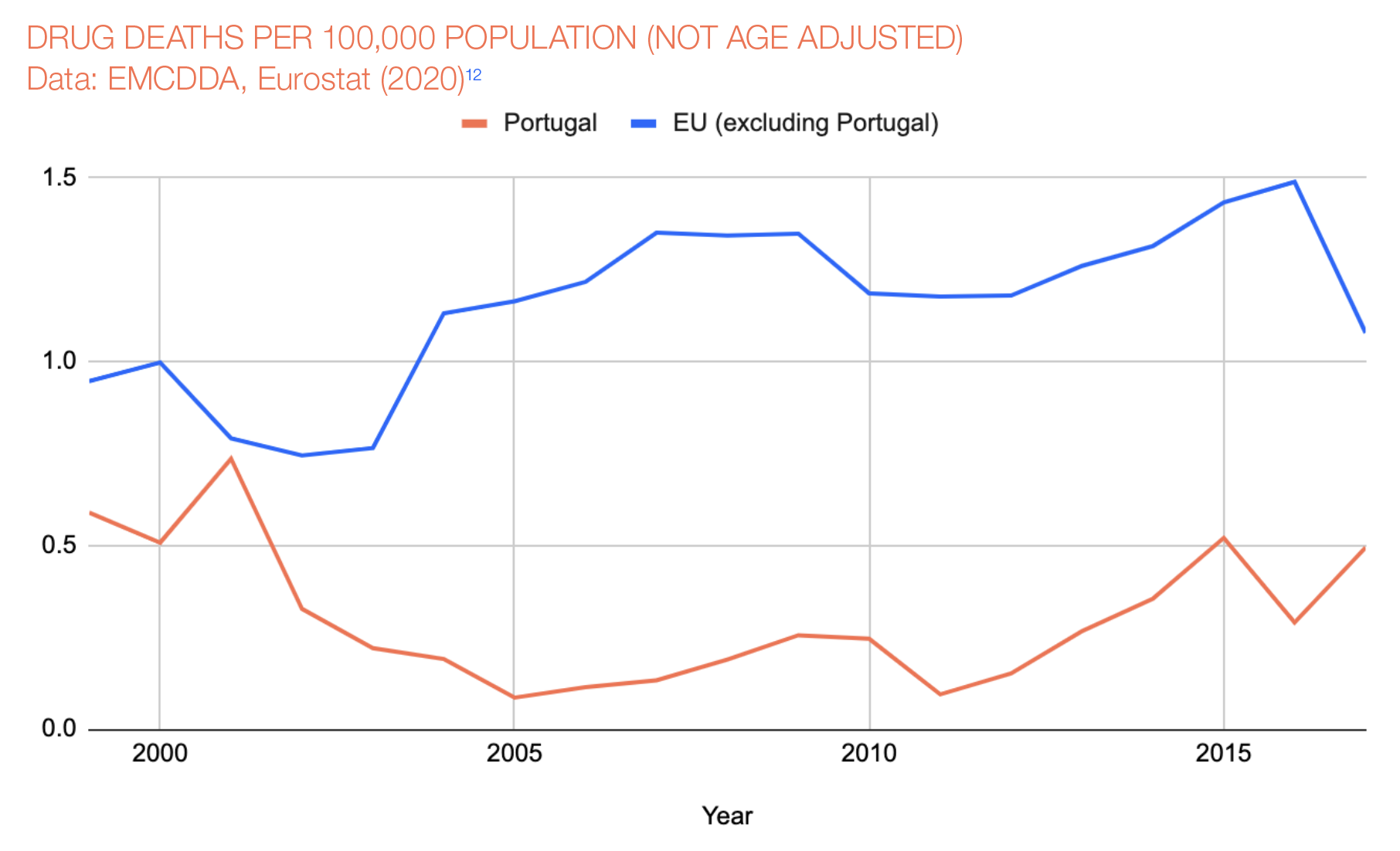
In the 1990s Portugal was facing a heroin epidemic that peaked in 1999 with 369 overdoses deaths. Instead of waging a drug war, Portugal moved to decriminalizing simple possessions and focused more on treatment. This resulted in a very rapid 80% decrease in overdoses. In 2016 there were 30 recorded overdoses deaths. Additionally, this lead to a significant drop in new HIV/AIDS cases contributed to injections, going from 52 percent (1,430 out of 2,758 cases) in 2000 to a low of 6 percent (77 out of 1,228) in 2015. Incarceration for drug offenses also decreased by 40%.
Spain, Italy, the Czech Republic, and a few other European countries have followed Portugal in the movement to decriminalize simple drug possessions. Uruguay in South America also never criminalized possession of drugs like most of the world did in the mid-20th century.
In 2016 the U.S. had an overdose rate of about 20 deaths per 100,000 compared to Portugal's .29, Spain's 1.04, the Czech Republic's .30, and Uruguay's 3.26. In 2017, the U.S. had about 72,000 overdose deaths. If the U.S. had a similar rate to Portugal, there would have been fewer than 800 overdose deaths.
However, simply decriminalizing drugs would probably not be effective in handling drug-related issues. An aspect that all these countries have that the U.S. doesn't is a considerable social safety net. These countries either have universal healthcare or a substantial public healthcare system.
Now if decriminalizing all drugs wasn't radical enough, another idea is government production and regulation of drugs. This could potentially have two benefits;
- Drugs would be "safer," as in the consumer knows what the product is. The consumer wouldn't have to worry about their cocaine or heroin being mixed with fentanyl.
- This could potentially hurt the current drug market. For example, why would someone buy heroin from cartel members when they can get it from a government-controlled center and know what they're getting?
Sources:
- John Hopkins School of Public Health - Health Effects of Marijuana
- MAPS - LSD-assisted Psychotherapy Follow-up
- John Hopkins - Magic Mushrooms Smoking
- John Hopkins - Hallucinogen Treats Cancer, Depression, Anxiety
- Link to Springer Article
- MAPS - Psilocybin for Smoking Cessation
- SAGE Journals - Psilocybin for Anxiety and Depression
- National Geographic - Drug Culture Around the World
- Our World in Data - Drug Use
- EMCDDA - Drug-Induced Deaths in Portugal
- EMCDDA - Drug Reports for Czechia
- EMCDDA - Drug Reports for Italy
- EMCDDA - Drug Reports for Spain
- Transform Drugs - Map of Drug Policy in Portugal
- Beckley Foundation - Lessons from Portugal: The Case for Drug Policy Reform
- Transform Drugs - Map of Drug Policies in Portugal